 |
| Click on image to enlarge. |
Scroll down for answer
*
*
*
*
*
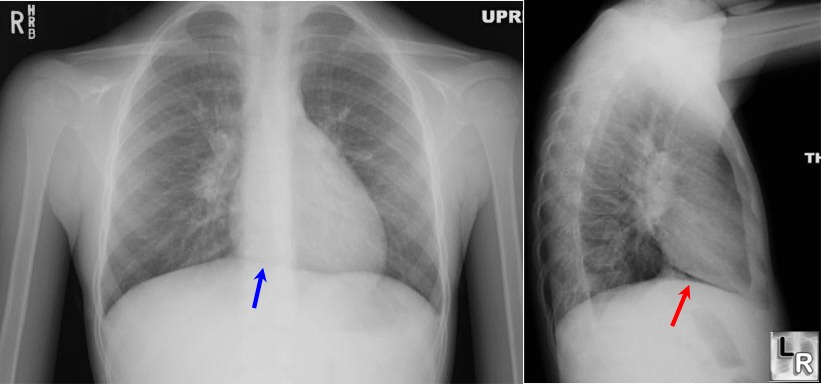
Pnuemomediastinum. Notice the free air in the neck on the chest x-ray.
Spontaneous, atraumatic, pneumomediastinum usually occurs when air leaks through small alveolar ruptures triggered by asthma or Valsalva maneuver and is a benign condition that resolves on its own in 2 to 15 days. Treatment includes analgesia and avoidance of maneuvers that increase pulmonary pressure, ie. Valsalva. Bronch is not indicated for screening of patients with isolated spontaneous pneumomediastinum. An esophageal study (contrast esophagography or esophagoscopy) is not indicated unless there is clinical concern for esophageal rupture. Rare complications of spontaneous pneumomediastinum that necessitate more aggressive care include tension pneumomediastinum and pneumopericardium.
Source
Saadoon, A. and Janahi, I. "Spontaneous pneumomediastinum in children and adolescents" Up to Date. May 2011.


















{kind=link}