This post is about an editorial comment by Dr. Richard Levitan on an article (1) about pulmonary critical care doctors performing intubations in the ICU (2). The study states that pulmonary critical care doctors can successfully perform this procedure. Dr. Levitan reports that intubation in elective anesthesia has a success rate between 98-99%, but when failure occurs the consequence can be catastrophic. The initial success rate of beginners is usually 50%, and it takes about 50 attempts in elective intubations to be 90% proficient.

The mystique of direct laryngoscopy, explains Dr. Levitan, is in the visual restrictions of the procedure. Due to this, difficult direct laryngoscopy can only be learned through trial and error, and each operator has to figure out the subtleties of the procedure. Time is also an issue, and the structures should be visualized within 10-15 seconds. As the beginner gains more experience, the brain pays more attention to the dominant eye while ignoring the visual field from non-dominant eye; a phenomenon called binocular suppression. Dr. Levitan goes on to explain the distance between the larynx and the eye, accommodation distance, is not necessarily determined by experience, but rather by age and intrinsic ocular issues.
This procedure can be learned more efficiently by understanding how visual restriction affects performance. This is learned by “using imaging from the operator’s perspective.” The best approach to learn this, as per Dr. Levitan, is by emphasizing the importance of:
- Epiglottoscopy
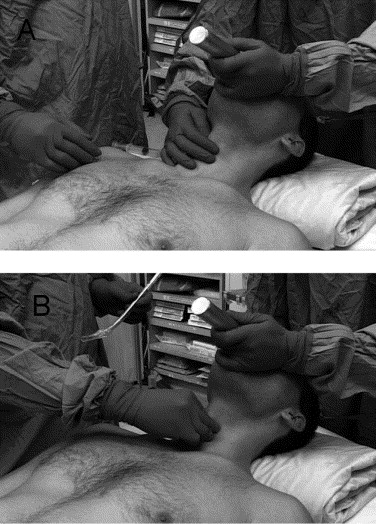
- Ear-to-sternal notch patient positioning
- Bi-manual laryngoscopy
- Straight-to-cuff stylet shaping
- In-depth understanding of laryngeal anatomy
It was no surprise to Dr. Levitan that doctors, if trained well, can perform this procedure adequately. But he also reports that in order to demystify the procedure, we must get better at teaching the best approach. Videolaryngoscopy is a helpful tool for teaching the operator’s perspective, Dr. Levitan then states that videolaryngoscopy is a great aid to augment initial direct laryngoscopy to improve patient safety.
The performance goal should not be plastic in the trachea, but first-pass success and avoidance of hypoxemia, regurgitation, hemodynamic instability, and other untoward effects that accompany repeated intubation attempts. -- LevitanWhat aspects of laryngoscopy do you usually emphasize when training novices? Do you use videolaryngoscopy when you train novices?
References:
- Vianello AM, et al. Management of tracheal intubation in the respiratory intensive care unit by pulmonary physicians. Respiratory Care. 2007 Jan;52(1):26-30. PMID: 17194314
- Levitan, RM, The Mystique of Direct Laryngoscopy. Respiratory Care. 2007 Jan;52(1):21-3. PMID: 17194312
For further learning on Direct Laryngoscopy please visit Dr. Weingart’s video on the Steps of laryngoscopy
Image source 1: http://www.sciencedirect.com/science/article/pii/S0196064406000709
Image source 2: http://www.airwaycam.com/Ocularity-and-Biomechanic-of-laryngoscopy.html
Image source 3: http://www.ojhas.org/issue38/2011-2-16.htm









